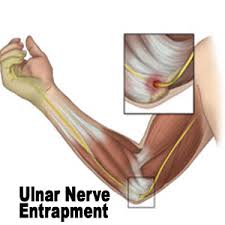
Cubital tunnel syndrome (CTS) is when there is increased pressure on the ulna nerve at the level of the elbow causing pain, pins and needles, numbness and weakness in the fingers.
Repetitive straining at this site can lead to scaring of tissues and put more pressure on the nerve. There are other causes including bony spurs (associated with arthritis of the elbow), cysts (ganglions), and associated conditions such as golfer’s elbows.
Pain, pins and needles, numbness and weakness in the fingers are the most common symptoms. Most commonly, the little finger and ring finger are affected (this is where the ulnar nerve supplies sensation to in the hand- see fig.1).
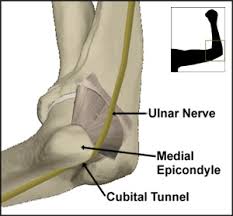
The specialist can usually diagnose it on clinical examination. A number of clinical tests can aid diagnosis including tapping over the ulnar nerve which sits just behind the inside part of the elbow. The specialist might refer you for nerve conduction studies to assess how much the nerve is compressed.
The treatment of this condition depends on how severely the patient is affected by the compression of the nerve and the nerve conduction study results. If the compression is severe, it is recommended that the nerve be decompressed in the form of surgery. This is a day-case procedure involving a general anaesthetic. A small cut is made on the inside part of the elbow. The tight bands pressing on the nerve are released and the pressure relieved. The main aim of surgery is to prevent further degeneration of the nerve (as if there is severe compression of the nerve, the nerve’s blood supply also gets compressed and the nerve supply to the muscle gets progressively weaker). After the surgery, the elbow is wrapped up in dressings. The patient is free to move the elbow as tolerated. A clinic appointment is made in two weeks to check on the wound healing, followed by referral to physiotherapy. Sometimes the ulnar nerve is found to be very mobile and it can dislocate out of it’s groove when the elbow is flexed. If this is the case, the nerve may need to be stabilised in a different position. This is called ulnar nerve transposition. If the ulnar nerve compression is mild, surgery may be avoided and physiotherapy and splints (see fig.4)